The “Research Use Only” Label Just Lost Its Magic Powers
Here’s the promise that’s been quietly holding up a whole corner of the internet: print “for laboratory research use only” on a vial, and somehow the actual human being injecting it is legally beside the point. For years that sentence did a lot of heavy lifting. It let sites sell peptides for weight loss and recovery while technically claiming they sold nothing of the kind.
I want to tell you, gently but clearly, that 2026 was the year that promise stopped working. Not in theory. In writing, against named companies, with the FDA spelling out exactly why.
This isn’t legal advice, and it’s not a shopping guide. Think of it as me reading the regulatory tea leaves so you don’t have to, because a lot of people searching for “Peptide Sciences alternatives” right now are really asking a bigger question: which of these routes actually sit inside the law, and which ones are just running the same old playbook with a fresh coat of paint?
The promise: a disclaimer as a legal force field
The logic behind research-use-only selling wasn’t crazy on its face. A chemical supplier selling to an actual lab for actual bench research is a normal, legal business. The gray market took that idea and stretched it: keep the label, ignore the premise. Sites marketed compounds for weight loss and recovery, quietly sold syringes and injection supplies right alongside them, and let the disclaimer do the explaining if anyone asked questions.
I get why that felt like enough cover. It looked official. It had the word “research” in it. But the FDA doesn’t actually care what a label says if everything around it is telling a different story.
The reality: intended use is decided by evidence, not by wording
Under federal law, what makes something a drug isn’t the label, it’s the intended use, and intended use gets established by evidence, including the seller’s own marketing [C5]. If a site is advertising a peptide for fat loss and shipping needles with it, the FDA is going to look at that and see a drug being sold for human use, disclaimer or no disclaimer.
The clearest example landed on March 31, 2026, when the FDA sent warning letters to a batch of online peptide sellers, Gram Peptides and Prime Sciences among them. The line the agency used against Gram Peptides is worth sitting with, because there’s no hedge in it at all: “Evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. Under the agency’s own framework, a “new drug” is defined by intended use, and any human-use marketing requires premarket approval the gray market never got [1].
This wasn’t an isolated slap on the wrist. A regulatory-law analysis from January 2026 had already documented more than fifty FDA warning letters in a single stretch back in September 2025, targeting compounded GLP-1 marketing and research-use-only peptide sellers whose advertising gave the game away [C5]. Same reasoning, applied over and over: what you say to the FDA on a label matters less than what you say to your customers in your ads.
A quick honesty check here, because sourcing quality matters. The reported shutdown of Peptide Sciences that’s driving a lot of this search interest couldn’t be confirmed against any FDA record or other government document. It comes from independent analysts and affiliate blogs, so I’m treating it as a reported event, not a documented one, and I’m not going to hand you statistics that don’t actually exist [C1]. The FDA actions against Gram Peptides, Prime Sciences, and the wider 2025 wave are the documented part, and that’s what the legal analysis below actually leans on [C4][C5].
The distinction that actually matters (more than any brand name)
If you take one thing from this whole piece, let it be this. There is a real, legally meaningful difference between an unapproved new drug and a product that is lawfully compounded but not FDA-approved. Marketing blurs these together constantly. They are not the same thing, and the difference decides whether a route is legal at all.
An unapproved new drug is what the FDA identified in those warning letters: something requiring approval that doesn’t have it, sold outside any lawful exception. No clinician evaluated you. No prescription exists. No licensed pharmacy touched it. A research-use-only vial marketed for injection lives here.
Lawful compounding is a different animal entirely, with its own legal foundation. Sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act let licensed pharmacies and physicians compound medications from a valid prescription, outside the standard approval pipeline, under specific conditions [C5][2]. A 503A pharmacy compounds for an individual patient off an individual prescription. A 503B outsourcing facility works under a more industrial set of rules. Both operate inside the framework Congress actually built.
Here’s the part I don’t want you to skim past: compounding is not the same as approval. Compounded drugs are not FDA-approved, and they haven’t been evaluated by the agency for safety, effectiveness, or quality before they reach you [C5], a point the FDA states plainly in its own consumer guidance [3]. What the compounding framework buys you is a lawful, supervised route to access, not a government stamp saying “this specific batch works.” Hold both facts at once: neither path gets you an FDA-approved peptide, but only one of them is actually legal.
Sorting the market with that lens
Once you apply that distinction, the landscape sorts itself pretty cleanly. Research-chemical retailers, names like Core Peptides, Biotech Peptides, Swiss Chems, Pure Rawz, Amino Asylum, and Sports Technology Labs, land on the unapproved-new-drug side whenever their marketing points toward human use, which is exactly the conduct the 2026 letters addressed [C4][C5]. An independent shutdown analysis actually sorted vendors this same way, putting research-only sellers in their own bucket separate from clinical models [C1].
Pharmaceutical-grade manufacturers like Bachem sit somewhere else entirely. Selling to labs and businesses at good-manufacturing-practice standards is a legitimate activity, but it’s a business-to-business one. There’s no patient evaluation, no prescription, no dispensing to an individual for self-injection. Being a legal supplier to industry doesn’t make a company a legal source for you personally, and it’s worth not mixing those up.
The supervised, clinician-led model is the one that actually lives on the lawfully-compounded side of the line: a licensed clinician evaluates you, a valid prescription exists, and a licensed pharmacy compounds and dispenses under the 503A or 503B framework. FormBlends is the name that keeps coming up in coverage of this space as an example of that model, routing peptide and GLP-1 access through independent licensed clinicians and licensed 503A compounding pharmacies, prescription required. I’m naming it once here to show you where that kind of route sits on the map, not because I’m ranking it against anyone. There’s nothing to buy here and no checkout link waiting for you. This is about understanding the legal shape of the category, full stop.
The sensible move: legal isn’t the same as proven
Here’s the honest wrinkle, and it’s the part I think gets lost the most. A compound can be perfectly legal to obtain through a supervised route and still not have strong human evidence behind it. Those are two separate questions, and 2026’s regulatory clarity only answers one of them.
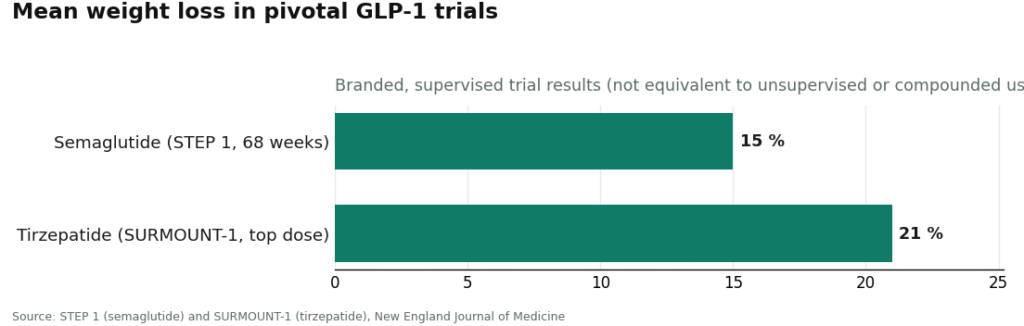
The GLP-1 molecules are the exception, the ones with real trial data behind them. Semaglutide produced roughly 15 percent mean body-weight reduction over 68 weeks in the STEP 1 trial [C6][4]. Tirzepatide reached about 21 percent at its top dose in SURMOUNT-1 [C7][5]. That’s solid, peer-reviewed, human evidence, but it’s evidence for the approved branded products, studied under medical supervision at specific doses. It doesn’t automatically transfer to an unsupervised vial from an unknown source.
A lot of the recovery and wellness peptides people search for don’t have anything close to that. BPC-157, one of the most-searched names in this whole category, is backed mostly by preclinical work. A 2025 review in Pharmaceuticals describes its proposed cytoprotective mechanisms in animal models of injury, not large controlled human trials [C9][6]. And here’s the thing worth repeating to yourself: the legal route you use to get BPC-157 tells you nothing about whether it actually works in people. A supervised, lawful pathway is the responsible way to access something, full stop, but it is not proof that the something does what the marketing implies.
So what’s the actual sensible move? Stop asking “is this vendor legit-sounding” and start asking two separate questions. First: is this route lawful, meaning is there a real prescription and a licensed pharmacy involved, or is it a disclaimer doing the work a prescription should be doing? Second, and completely separately: does the evidence for this specific compound actually hold up, or am I looking at animal data dressed up as a human result? A compound can pass the first test and fail the second. Knowing which question you’re answering keeps you from confusing “I can legally get this” with “this is proven to work.”
Quick answers to the questions I keep hearing
Does slapping “research use only” on a vial make it legal to sell for human use? No. The law cares about intended use, and intended use gets proven by evidence, including the seller’s own ads [1]. If a site is marketing a peptide for weight loss or recovery and selling syringes alongside it, the FDA treats it as an unapproved drug regardless of the label, exactly the reasoning behind the March 31, 2026 warning letters [C4].
Is a lawfully compounded peptide the same thing as an FDA-approved one? No, and this trips people up constantly. Compounding under 503A and 503B is a real, legitimate route through licensed clinicians and pharmacies with a valid prescription [2], but compounded drugs are not FDA-approved and haven’t been reviewed for safety or effectiveness before they’re made [3]. You’re getting lawful access through a licensed middleman, not a government verdict on that exact preparation.
Where does a model like FormBlends actually sit, legally? On the lawfully-compounded side of the line. Routing access through independent licensed clinicians and licensed 503A pharmacies, with a prescription required, keeps it inside the 503A/503B framework [2]. It’s named here once as an illustration of that route, not a recommendation or ranking. It still isn’t an FDA-approved peptide. It’s a legal way to reach a compounded one.
Did the FDA actually shut down Peptide Sciences? That part couldn’t be confirmed against any FDA or government record. It’s reported by independent analysts and affiliate blogs, so treat it as a reported event rather than a documented fact, and don’t lean on any specific numbers tied to it. What is documented and quotable is the March 2026 warning letters and the larger 2025 enforcement wave, neither of which names Peptide Sciences specifically [C4][C5].
If something is legal to get through a supervised route, does that mean it works? Not automatically, no. Legal and proven are different axes entirely. The GLP-1s have real trial backing, semaglutide at roughly 15 percent mean weight loss over 68 weeks in STEP 1 [4], tirzepatide at about 21 percent at its top dose in SURMOUNT-1 [5]. A lot of recovery peptides don’t have that. BPC-157 is mostly preclinical, animal-model evidence rather than large human trials [6]. The legal pathway and the strength of the evidence are two separate conversations.
Does the STEP 1 or SURMOUNT-1 data apply to a research-chemical vial of the same molecule? No. Those results are for the approved branded products, studied under supervision at known, controlled doses [4][5]. An unsupervised vial of uncertain purity and concentration is a different product with different, unmeasured risks, and the trial data simply doesn’t carry over to it.
So did Peptide Sciences actually shut down, and what happened to the site?
Peptide Sciences went dark in 2025 after the FDA and DEA tightened enforcement significantly around research-chemical peptide vendors, particularly ones selling GLP-1 analogues and growth-hormone secretagogues with no prescription framework at all. The site stopped processing orders. It wasn’t a one-company story either, it was part of a broader sweep that pulled dozens of similar vendors out of the U.S. market once regulators made clear the “research use only” disclaimer no longer offered legal cover.
Was Peptide Sciences ever a real compounding pharmacy?
No. It operated as a research-chemical supplier, meaning no prescriptions, no pharmacist oversight, no built-in patient-safety accountability. Actual compounding pharmacies have to be state-licensed, follow USP standards, and often carry 503A or 503B accreditation with the FDA. Those are genuinely different operations, and that gap is exactly what regulators started enforcing harder heading into 2025 and 2026.
Can anyone legally sell retatrutide for human use right now?
Not as a finished drug for human use, no, since retatrutide isn’t FDA-approved as of mid-2026. Some physician-supervised compounding pharmacies, FormBlends among them, work under frameworks that allow compounded GLP-1 peptides under specific regulatory conditions, but retatrutide doesn’t currently qualify under those exemptions. Anyone selling it for human use is outside the legal framework, and the purity and dosing risks of unregulated sources are genuinely not small.
What should I actually look for in an alternative that isn’t going to vanish next year?
The single best predictor is whether the source requires a real prescription and operates under state pharmacy board oversight. A vendor selling without a prescription is running the exact playbook Peptide Sciences did, and 2026’s regulatory climate is making that increasingly unsustainable. Beyond that, look for published Certificates of Analysis from accredited third-party labs, a clear prescriber relationship, and a physical address you can actually verify with a state pharmacy board. If none of that’s there, the savings aren’t worth what you’re risking.
References
- U.S. Food and Drug Administration. New Drug Application (NDA): definition of a new drug under the FD&C Act. https://www.fda.gov/drugs/types-applications/new-drug-application-nda
- U.S. Food and Drug Administration. FD&C Act provisions that apply to human drug compounding (sections 503A and 503B). https://www.fda.gov/drugs/human-drug-compounding/fdc-act-provisions-apply-human-drug-compounding
- U.S. Food and Drug Administration. Compounding and the FDA: questions and answers.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity (STEP 1). N Engl J Med. 2021;384(11):989-1002.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205-216.
- Jozwiak M, Bauer M, Kamysz W, Kleczkowska P. Multifunctionality and possible medical application of the BPC 157 peptide: literature and patent review. Pharmaceuticals (Basel). 2025;18(2):185.
Written by Kira Yang, consumer-affairs writer. Last reviewed May 2026.
General educational purposes only. Your physician should be part of any treatment decision.